Everything You Want To Know About Heel Serious Pain
Overview

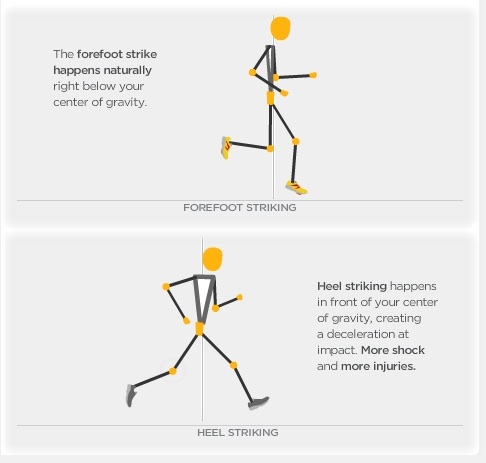
When walking, your heels repeatedly hit the ground with considerable force. They have to be able to absorb the impact and provide a firm support for the weight of the body. When pain develops in the heel, it can be very disabling, making every step a problem, affecting your posture. There are various types of heel pain. Some of the most common are heel spurs (plantar fasciitis); heel bursitis and heel bumps.
Causes
Pain in the foot can be due to a problem in any part of the foot. Bones, ligaments, tendons, muscles, fascia, toenail beds, nerves, blood vessels, or skin can be the source of foot pain. The cause of foot pain can be narrowed down by location and by considering some of the most common causes of foot pain. Plantar fasciitis is the most common cause of heel pain. The plantar fascia, a band of tough tissue connecting the heel bone to the toes, becomes irritated or inflamed. Heel pain, worst in the morning when getting out of bed, is the most common symptom. Arch pain may also be present.
Symptoms
Pain in the heel can be caused by many things. The commonest cause is plantar fascitis. Other causes include, being overweight, constantly being on your feet, especially on a hard surface like concrete and wearing hard-soled footwear, thinning or weakness of the fat pads of the heel, injury to the bones or padding of the heel, arthritis in the ankle or heel (subtalar) joint, irritation of the nerves on the inner or outer sides of the heel, fracture of the heel bone (calcaneum).
Diagnosis
After you have described your foot symptoms, your doctor will want to know more details about your pain, your medical history and lifestyle, including. Whether your pain is worse at specific times of the day or after specific activities. Any recent injury to the area. Your medical and orthopedic history, especially any history of diabetes, arthritis or injury to your foot or leg. Your age and occupation. Your recreational activities, including sports and exercise programs. The type of shoes you usually wear, how well they fit, and how frequently you buy a new pair. Your doctor will examine you, including. An evaluation of your gait. While you are barefoot, your doctor will ask you to stand still and to walk in order to evaluate how your foot moves as you walk. An examination of your feet. Your doctor may compare your feet for any differences between them. Then your doctor may examine your painful foot for signs of tenderness, swelling, discoloration, muscle weakness and decreased range of motion. A neurological examination. The nerves and muscles may be evaluated by checking strength, sensation and reflexes. In addition to examining you, your health care professional may want to examine your shoes. Signs of excessive wear in certain parts of a shoe can provide valuable clues to problems in the way you walk and poor bone alignment. Depending on the results of your physical examination, you may need foot X-rays or other diagnostic tests.
Non Surgical Treatment
Calf stretch, Heel cups/lifts, ice, night splint, physical therapy, activity modification. Sometimes immobilization in a cast or boot may be necessary. Topical creams, such as Voltaren or Ketoprofen, have been found to have some benefit. In some cases, the tendon may become degenerative (tendonosis). In these instances, treatment is more difficult. Prolonged periods of immobilization and physical therapy may be required. In resistant cases, surgical debridement of the tendon may be necessary. Rarely does a symptomatic achilles tendon rupture. Most achilles ruptures are not associated with prodromal symptoms. Achilles ruptures are more common in men and "weekend warriors," ie middle aged men who like to play sports (soccer, softball, basketball) on the weekends.
Surgical Treatment
With the advancements in technology and treatments, if you do need to have surgery for the heel, it is very minimal incision that?s done. And the nice thing is your recovery period is short and you should be able to bear weight right after the surgery. This means you can get back to your weekly routine in just a few weeks. Recovery is a lot different than it used to be and a lot of it is because of doing a minimal incision and decreasing trauma to soft tissues, as well as even the bone. So if you need surgery, then your recovery period is pretty quick.
deelsonheels
Prevention
It is not always possible to prevent heel pain, but there are measures you can take to help avoid further episodes. Being overweight can place excess pressure and strain on your feet, particularly on your heels. This increases the risk of damaging your feet and heels. If you are overweight, losing weight and maintaining a healthy weight by combining regular exercise with a healthy, balanced diet can be beneficial for your feet. You can calculate your body mass index (BMI) to find out whether you are a healthy weight for your height and build. To work out your BMI, divide your weight in kilograms by your height in metres squared. A BMI of less than 18.5 means that you are underweight, 18.5-24.9 means that your weight is healthy, 25-29 means that you are overweight, 30-40 means that you are obese, over 40 means that you are morbidly obese. You can also use the BMI healthy weight calculator to work out your BMI.
When walking, your heels repeatedly hit the ground with considerable force. They have to be able to absorb the impact and provide a firm support for the weight of the body. When pain develops in the heel, it can be very disabling, making every step a problem, affecting your posture. There are various types of heel pain. Some of the most common are heel spurs (plantar fasciitis); heel bursitis and heel bumps.
Causes
Pain in the foot can be due to a problem in any part of the foot. Bones, ligaments, tendons, muscles, fascia, toenail beds, nerves, blood vessels, or skin can be the source of foot pain. The cause of foot pain can be narrowed down by location and by considering some of the most common causes of foot pain. Plantar fasciitis is the most common cause of heel pain. The plantar fascia, a band of tough tissue connecting the heel bone to the toes, becomes irritated or inflamed. Heel pain, worst in the morning when getting out of bed, is the most common symptom. Arch pain may also be present.
Symptoms
Pain in the heel can be caused by many things. The commonest cause is plantar fascitis. Other causes include, being overweight, constantly being on your feet, especially on a hard surface like concrete and wearing hard-soled footwear, thinning or weakness of the fat pads of the heel, injury to the bones or padding of the heel, arthritis in the ankle or heel (subtalar) joint, irritation of the nerves on the inner or outer sides of the heel, fracture of the heel bone (calcaneum).
Diagnosis
After you have described your foot symptoms, your doctor will want to know more details about your pain, your medical history and lifestyle, including. Whether your pain is worse at specific times of the day or after specific activities. Any recent injury to the area. Your medical and orthopedic history, especially any history of diabetes, arthritis or injury to your foot or leg. Your age and occupation. Your recreational activities, including sports and exercise programs. The type of shoes you usually wear, how well they fit, and how frequently you buy a new pair. Your doctor will examine you, including. An evaluation of your gait. While you are barefoot, your doctor will ask you to stand still and to walk in order to evaluate how your foot moves as you walk. An examination of your feet. Your doctor may compare your feet for any differences between them. Then your doctor may examine your painful foot for signs of tenderness, swelling, discoloration, muscle weakness and decreased range of motion. A neurological examination. The nerves and muscles may be evaluated by checking strength, sensation and reflexes. In addition to examining you, your health care professional may want to examine your shoes. Signs of excessive wear in certain parts of a shoe can provide valuable clues to problems in the way you walk and poor bone alignment. Depending on the results of your physical examination, you may need foot X-rays or other diagnostic tests.
Non Surgical Treatment
Calf stretch, Heel cups/lifts, ice, night splint, physical therapy, activity modification. Sometimes immobilization in a cast or boot may be necessary. Topical creams, such as Voltaren or Ketoprofen, have been found to have some benefit. In some cases, the tendon may become degenerative (tendonosis). In these instances, treatment is more difficult. Prolonged periods of immobilization and physical therapy may be required. In resistant cases, surgical debridement of the tendon may be necessary. Rarely does a symptomatic achilles tendon rupture. Most achilles ruptures are not associated with prodromal symptoms. Achilles ruptures are more common in men and "weekend warriors," ie middle aged men who like to play sports (soccer, softball, basketball) on the weekends.
Surgical Treatment
With the advancements in technology and treatments, if you do need to have surgery for the heel, it is very minimal incision that?s done. And the nice thing is your recovery period is short and you should be able to bear weight right after the surgery. This means you can get back to your weekly routine in just a few weeks. Recovery is a lot different than it used to be and a lot of it is because of doing a minimal incision and decreasing trauma to soft tissues, as well as even the bone. So if you need surgery, then your recovery period is pretty quick.
deelsonheels
Prevention
It is not always possible to prevent heel pain, but there are measures you can take to help avoid further episodes. Being overweight can place excess pressure and strain on your feet, particularly on your heels. This increases the risk of damaging your feet and heels. If you are overweight, losing weight and maintaining a healthy weight by combining regular exercise with a healthy, balanced diet can be beneficial for your feet. You can calculate your body mass index (BMI) to find out whether you are a healthy weight for your height and build. To work out your BMI, divide your weight in kilograms by your height in metres squared. A BMI of less than 18.5 means that you are underweight, 18.5-24.9 means that your weight is healthy, 25-29 means that you are overweight, 30-40 means that you are obese, over 40 means that you are morbidly obese. You can also use the BMI healthy weight calculator to work out your BMI.
Do Fallen Arches Need Surgery?
Overview

The human foot is a complex structure that absorbs shock every time we take a step. The foot has to adapt to a variety of movements during different forms of activities such as walking, running and climbing steps. The foot is made up of many different joints, ligaments and muscles which have to work together to allow us to move and balance. The arch of the foot plays and important role in absorbing shock and preventing over stressing of the foot muscles and bones. In this article, we shall briefly discuss flat feet and fallen arches. These two conditions are closely related to each other and can increase the risk of overuse injury to the foot. They can also cause overload of more proximal structures such as ankles, shins, knees and the lower back.
Causes
Fallen arches can be the result of other conditions such as overuse, stretching or tearing of the posterior tibial tendon (which attaches to a bone in the foot and runs up the calf of the lower leg at a tension which pulls up the arch) which reduces its ability to maintain tension in the tendon. Whether or not the condition is caused by overpronation, this is the likely outcome for runners, whose arches are no longer strong enough to take the constant strain of bearing the body?s weight on impact, causing joint, postural and muscular problems.
Symptoms
Fallen arches symptoms may include the following. Being unable to slip fingers underneath arches. Inwards rolling of foot and ankle when running. Knee problems due to lack of support from feet.
Diagnosis
People who have flat feet without signs or symptoms that bother them do not generally have to see a doctor or podiatrist about them. However, if any of the following occur, you should see your GP or a podiatrist. The fallen arches (flat feet) have developed recently. You experience pain in your feet, ankles or lower limbs. Your unpleasant symptoms do not improve with supportive, well-fitted shoes. Either or both feet are becoming flatter. Your feet feel rigid (stiff). Your feet feel heavy and unwieldy. Most qualified health care professionals can diagnose flat feet just by watching the patient stand, walk and examining his/her feet. A doctor will also look at the patient's medical history. The feet will be observed from the front and back. The patient may be asked to stand on tip-toe while the doctor examines the shape and functioning of each foot. In some cases the physician may order an X-ray, CT (computed tomography) scan, or MRI (magnetic resonance imaging) scan.
Is flat footedness genetic?
Non Surgical Treatment
Heel cord stretching is an important part of treatment, as a tight Achilles tendon tends to pronate the foot. Orthotics (inserts or insoles, often custom-made) may be used. These usually contain a heel wedge to correct calcaneovalgus deformity, and an arch support. This is the usual treatment for flexible Pes Planus (if treatment is needed). A suitable insole can help to correct the deformity while it is worn. Possibly it may prevent progression of flat feet, or may reduce symptoms. However, the effectiveness of arch support insoles is uncertain. Arch supports used without correcting heel cord contracture can make symptoms worse. In patients with fixed Pes planus or arthropathy, customised insoles may relieve symptoms. Reduce contributing factors, wear shoes with low heels and wide toes. Lose weight if appropriate. Do exercises to strengthen foot muscles - walking barefoot (if appropriate), toe curls (flexing toes) and heel raises (standing on tiptoe).
Surgical Treatment

Surgical correction is dependent on the severity of symptoms and the stage of deformity. The goals of surgery are to create a more functional and stable foot. There are multiple procedures available to the surgeon and it may take several to correct a flatfoot deformity. Stage one deformities usually respond to conservative or non-surgical therapy such as anti-inflammatory medication, casting, functional orthotics or a foot ankle orthosis called a Richie Brace. If these modalities are unsuccessful surgery is warranted. Usually surgical treatment begins with removal of inflammatory tissue and repair of the posterior tibial tendon. A tendon transfer is performed if the posterior tibial muscle is weak or the tendon is badly damaged. The most commonly used tendon is the flexor digitorum longus tendon. This tendon flexes or moves the lesser toes downward. The flexor digitorum longus tendon is utilized due to its close proximity to the posterior tibial tendon and because there are minimal side effects with its loss. The remainder of the tendon is sutured to the flexor hallucis longus tendon that flexes the big toe so that little function is loss. Stage two deformities are less responsive to conservative therapies that can be effective in mild deformities. Bone procedures are necessary at this stage in order to recreate the arch and stabilize the foot. These procedures include isolated fusion procedures, bone grafts, and/or the repositioning of bones through cuts called osteotomies. The realigned bones are generally held in place with screws, pins, plates, or staples while the bone heals. A tendon transfer may or may not be utilized depending on the condition of the posterior tibial tendon. Stage three deformities are better treated with surgical correction, in healthy patients. Patients that are unable to tolerate surgery or the prolonged healing period are better served with either arch supports known as orthotics or bracing such as the Richie Brace. Surgical correction at this stage usually requires fusion procedures such as a triple or double arthrodesis. This involves fusing the two or three major bones in the back of the foot together with screws or pins. The most common joints fused together are the subtalar joint, talonavicular joint, and the calcaneocuboid joint. By fusing the bones together the surgeon is able to correct structural deformity and alleviate arthritic pain. Tendon transfer procedures are usually not beneficial at this stage. Stage four deformities are treated similarly but with the addition of fusing the ankle joint.
Prevention
Sit up straight in a chair with your feet flat on the ground. Scrunch up the toes of one foot as if you are trying to grab hold of the floor then use your toes to drag your foot a small distance forwards. Do this a couple of times on each foot, but don?t use your leg muscles to push your foot forward -- the movement should come solely from the muscles in your feet. Sit in a chair and place a cleaning cloth, towel or small ball on the floor at your feet. Use the toes of one foot to grasp the object and lift it off the floor. This action will require you to clench your toes and contract your arch. Once you have lifted the object a little way off the floor, try to throw it in the air and catch it by stretching your toes and arch out and upwards. Repeat the exercise several times on both feet. Sit on the floor with your legs straight out in front of you then bend your knees out to either side and place the soles of your feet together so your legs form a diamond. Hold on to your ankles and, keeping your heels together at all times, separate your feet so your toes point out to either side. Open and close your feet in this way several times, making sure your little toes stay in contact with the floor throughout the exercise. Starting in the same position, try separating your heels, keeping your toes together at all times.
The human foot is a complex structure that absorbs shock every time we take a step. The foot has to adapt to a variety of movements during different forms of activities such as walking, running and climbing steps. The foot is made up of many different joints, ligaments and muscles which have to work together to allow us to move and balance. The arch of the foot plays and important role in absorbing shock and preventing over stressing of the foot muscles and bones. In this article, we shall briefly discuss flat feet and fallen arches. These two conditions are closely related to each other and can increase the risk of overuse injury to the foot. They can also cause overload of more proximal structures such as ankles, shins, knees and the lower back.
Causes
Fallen arches can be the result of other conditions such as overuse, stretching or tearing of the posterior tibial tendon (which attaches to a bone in the foot and runs up the calf of the lower leg at a tension which pulls up the arch) which reduces its ability to maintain tension in the tendon. Whether or not the condition is caused by overpronation, this is the likely outcome for runners, whose arches are no longer strong enough to take the constant strain of bearing the body?s weight on impact, causing joint, postural and muscular problems.
Symptoms
Fallen arches symptoms may include the following. Being unable to slip fingers underneath arches. Inwards rolling of foot and ankle when running. Knee problems due to lack of support from feet.
Diagnosis
People who have flat feet without signs or symptoms that bother them do not generally have to see a doctor or podiatrist about them. However, if any of the following occur, you should see your GP or a podiatrist. The fallen arches (flat feet) have developed recently. You experience pain in your feet, ankles or lower limbs. Your unpleasant symptoms do not improve with supportive, well-fitted shoes. Either or both feet are becoming flatter. Your feet feel rigid (stiff). Your feet feel heavy and unwieldy. Most qualified health care professionals can diagnose flat feet just by watching the patient stand, walk and examining his/her feet. A doctor will also look at the patient's medical history. The feet will be observed from the front and back. The patient may be asked to stand on tip-toe while the doctor examines the shape and functioning of each foot. In some cases the physician may order an X-ray, CT (computed tomography) scan, or MRI (magnetic resonance imaging) scan.
Is flat footedness genetic?
Non Surgical Treatment
Heel cord stretching is an important part of treatment, as a tight Achilles tendon tends to pronate the foot. Orthotics (inserts or insoles, often custom-made) may be used. These usually contain a heel wedge to correct calcaneovalgus deformity, and an arch support. This is the usual treatment for flexible Pes Planus (if treatment is needed). A suitable insole can help to correct the deformity while it is worn. Possibly it may prevent progression of flat feet, or may reduce symptoms. However, the effectiveness of arch support insoles is uncertain. Arch supports used without correcting heel cord contracture can make symptoms worse. In patients with fixed Pes planus or arthropathy, customised insoles may relieve symptoms. Reduce contributing factors, wear shoes with low heels and wide toes. Lose weight if appropriate. Do exercises to strengthen foot muscles - walking barefoot (if appropriate), toe curls (flexing toes) and heel raises (standing on tiptoe).
Surgical Treatment
Surgical correction is dependent on the severity of symptoms and the stage of deformity. The goals of surgery are to create a more functional and stable foot. There are multiple procedures available to the surgeon and it may take several to correct a flatfoot deformity. Stage one deformities usually respond to conservative or non-surgical therapy such as anti-inflammatory medication, casting, functional orthotics or a foot ankle orthosis called a Richie Brace. If these modalities are unsuccessful surgery is warranted. Usually surgical treatment begins with removal of inflammatory tissue and repair of the posterior tibial tendon. A tendon transfer is performed if the posterior tibial muscle is weak or the tendon is badly damaged. The most commonly used tendon is the flexor digitorum longus tendon. This tendon flexes or moves the lesser toes downward. The flexor digitorum longus tendon is utilized due to its close proximity to the posterior tibial tendon and because there are minimal side effects with its loss. The remainder of the tendon is sutured to the flexor hallucis longus tendon that flexes the big toe so that little function is loss. Stage two deformities are less responsive to conservative therapies that can be effective in mild deformities. Bone procedures are necessary at this stage in order to recreate the arch and stabilize the foot. These procedures include isolated fusion procedures, bone grafts, and/or the repositioning of bones through cuts called osteotomies. The realigned bones are generally held in place with screws, pins, plates, or staples while the bone heals. A tendon transfer may or may not be utilized depending on the condition of the posterior tibial tendon. Stage three deformities are better treated with surgical correction, in healthy patients. Patients that are unable to tolerate surgery or the prolonged healing period are better served with either arch supports known as orthotics or bracing such as the Richie Brace. Surgical correction at this stage usually requires fusion procedures such as a triple or double arthrodesis. This involves fusing the two or three major bones in the back of the foot together with screws or pins. The most common joints fused together are the subtalar joint, talonavicular joint, and the calcaneocuboid joint. By fusing the bones together the surgeon is able to correct structural deformity and alleviate arthritic pain. Tendon transfer procedures are usually not beneficial at this stage. Stage four deformities are treated similarly but with the addition of fusing the ankle joint.
Prevention
Sit up straight in a chair with your feet flat on the ground. Scrunch up the toes of one foot as if you are trying to grab hold of the floor then use your toes to drag your foot a small distance forwards. Do this a couple of times on each foot, but don?t use your leg muscles to push your foot forward -- the movement should come solely from the muscles in your feet. Sit in a chair and place a cleaning cloth, towel or small ball on the floor at your feet. Use the toes of one foot to grasp the object and lift it off the floor. This action will require you to clench your toes and contract your arch. Once you have lifted the object a little way off the floor, try to throw it in the air and catch it by stretching your toes and arch out and upwards. Repeat the exercise several times on both feet. Sit on the floor with your legs straight out in front of you then bend your knees out to either side and place the soles of your feet together so your legs form a diamond. Hold on to your ankles and, keeping your heels together at all times, separate your feet so your toes point out to either side. Open and close your feet in this way several times, making sure your little toes stay in contact with the floor throughout the exercise. Starting in the same position, try separating your heels, keeping your toes together at all times.
Leg Length Discrepancy Treatment For Adults
Overview
Leg length discrepancy is an orthopaedic problem that usually appears in childhood, in which one's two legs are of unequal lengths. Often abbreviated as ?LLD,' leg length discrepancy may be caused by or associated with a number of other orthopaedic or medical conditions, but is generally treated in a similar fashion, regardless of cause and depending on severity. Leg length discrepancy is sometimes divided up into 'true LLD' and 'functional LLD.' Functional LLD occurs when the legs are actually equal in length, but some other condition, such as pelvic obliquity (a tilt in the position of the pelvis), creates the appearance of legs of different lengths.
Causes
Common causes include bone infection, bone diseases, previous injuries, or broken bones. Other causes may include birth defects, arthritis where there is a loss of articular surface, or neurological conditions.
Symptoms
Many people walk around with LLD?s of up to 2 cm. and not even know it. However, discrepancies above 2 cm. becomes more noticeable, and a slight limp is present. But even up to 3 cm. a small lift compensates very well, and many patients are quite happy with this arrangement. Beyond 3 cm. however, the limp is quite pronounced, and medical care is often sought at that point. Walking with a short leg gait is not only unsightly, but increases energy expenditure during ambulation. It could also put more stress on the long leg, and causes functional scoliosis. Where the discrepancy is more severe, walking becomes grotesque or virtually impossible.
Diagnosis
Asymmetry is a clue that a LLD is present. The center of gravity will shift to the short limb side and patients will try to compensate, displaying indications such as pelvic tilt, lumbar scoliosis, knee flexion, or unilateral foot pronation. Asking simple questions such as, "Do you favor one leg over the other?" or, "Do you find it uncomfortable to stand?" may also provide some valuable information. Performing a gait analysis will yield some clues as to how the patient compensates during ambulation. Using plantar pressure plates can indicate load pressure differences between the feet. It is helpful if the gait analysis can be video-recorded and played back in slow motion to catch the subtle aspects of movement.
Non Surgical Treatment
A personalized approach to leg length discrepancy treatment works best for each patient. Your child's doctor will consider many factors when deciding on a course of treatment for this condition. Such factors can include your child's age, extent of the leg length discrepancy, medical history, how your child tolerates certain treatments and procedures, your child's health and prognosis, growth rate, and parental preferences. There is no cookie cutter treatment for each child, or even each centimeter of leg difference. Once all of these factors have been carefully considered, your child's physician will come up with an appropriate course of care. In situations of a very small leg length discrepancy, no treatment, only periodic medical evaluation, may be necessary.

what can i do to get taller?
Surgical Treatment
Shortening techniques can be used after skeletal maturity to achieve leg length equality. Shortening can be done in the proximal femur using a blade plate or hip screw, in the mid-diaphysis of the femur using a closed intramedullary (IM) technique, or in the tibia. Shortening is an accurate technique and involves a much shorter convalescence than lengthening techniques. Quadriceps weakness may occur with femoral shortenings, especially if a mid-diaphyseal shortening of greater than 10% is done. If the femoral shortening is done proximally, no significant weakness should result. Tibial shortening can be done, but there may be a residual bulkiness to the leg, and risks of nonunion and compartment syndrome are higher. If a tibial shortening is done, shortening over an IM nail and prophylactic compartment release are recommended. We limit the use of shortenings to 4 to 5 cm leg length inequality in patients who are skeletally mature.
Leg length discrepancy is an orthopaedic problem that usually appears in childhood, in which one's two legs are of unequal lengths. Often abbreviated as ?LLD,' leg length discrepancy may be caused by or associated with a number of other orthopaedic or medical conditions, but is generally treated in a similar fashion, regardless of cause and depending on severity. Leg length discrepancy is sometimes divided up into 'true LLD' and 'functional LLD.' Functional LLD occurs when the legs are actually equal in length, but some other condition, such as pelvic obliquity (a tilt in the position of the pelvis), creates the appearance of legs of different lengths.
Causes
Common causes include bone infection, bone diseases, previous injuries, or broken bones. Other causes may include birth defects, arthritis where there is a loss of articular surface, or neurological conditions.
Symptoms
Many people walk around with LLD?s of up to 2 cm. and not even know it. However, discrepancies above 2 cm. becomes more noticeable, and a slight limp is present. But even up to 3 cm. a small lift compensates very well, and many patients are quite happy with this arrangement. Beyond 3 cm. however, the limp is quite pronounced, and medical care is often sought at that point. Walking with a short leg gait is not only unsightly, but increases energy expenditure during ambulation. It could also put more stress on the long leg, and causes functional scoliosis. Where the discrepancy is more severe, walking becomes grotesque or virtually impossible.
Diagnosis
Asymmetry is a clue that a LLD is present. The center of gravity will shift to the short limb side and patients will try to compensate, displaying indications such as pelvic tilt, lumbar scoliosis, knee flexion, or unilateral foot pronation. Asking simple questions such as, "Do you favor one leg over the other?" or, "Do you find it uncomfortable to stand?" may also provide some valuable information. Performing a gait analysis will yield some clues as to how the patient compensates during ambulation. Using plantar pressure plates can indicate load pressure differences between the feet. It is helpful if the gait analysis can be video-recorded and played back in slow motion to catch the subtle aspects of movement.
Non Surgical Treatment
A personalized approach to leg length discrepancy treatment works best for each patient. Your child's doctor will consider many factors when deciding on a course of treatment for this condition. Such factors can include your child's age, extent of the leg length discrepancy, medical history, how your child tolerates certain treatments and procedures, your child's health and prognosis, growth rate, and parental preferences. There is no cookie cutter treatment for each child, or even each centimeter of leg difference. Once all of these factors have been carefully considered, your child's physician will come up with an appropriate course of care. In situations of a very small leg length discrepancy, no treatment, only periodic medical evaluation, may be necessary.
what can i do to get taller?
Surgical Treatment
Shortening techniques can be used after skeletal maturity to achieve leg length equality. Shortening can be done in the proximal femur using a blade plate or hip screw, in the mid-diaphysis of the femur using a closed intramedullary (IM) technique, or in the tibia. Shortening is an accurate technique and involves a much shorter convalescence than lengthening techniques. Quadriceps weakness may occur with femoral shortenings, especially if a mid-diaphyseal shortening of greater than 10% is done. If the femoral shortening is done proximally, no significant weakness should result. Tibial shortening can be done, but there may be a residual bulkiness to the leg, and risks of nonunion and compartment syndrome are higher. If a tibial shortening is done, shortening over an IM nail and prophylactic compartment release are recommended. We limit the use of shortenings to 4 to 5 cm leg length inequality in patients who are skeletally mature.
Apparent Leg Length Discrepancy Causes
Overview
In growing children, legs can be made equal or nearly equal in length with a relatively simple surgical procedure. This procedure slows down the growth of the longer leg at one or two growth sites. Your physician can tell you how much equalization can be gained by this procedure. The procedure is performed under X-ray control through very small incisions in the knee area. This procedure will not cause an immediate correction in length. Instead, the limb length discrepancy will gradually decrease as the opposite extremity continues to grow and "catch up." Timing of the procedure is critical. The goal is to reach equal leg length by the time growth normally ends. This is usually in the mid-to-late teenage years. Disadvantages of this option include the possibility of slight over-correction or under-correction of the limb length discrepancy. In addition, the patient's adult height will be less than if the shorter leg had been lengthened. Correction of significant limb length discrepancy by this method may make a patient's body look slightly disproportionate because of the shorter leg. In some cases the longer leg can be shortened, but a major shortening may weaken the muscles of the leg. In the thighbone (femur), a maximum of 3 inches can be shortened. In the shinbone, a maximum of 2 inches can be shortened.
Causes
Limb-length conditions can result from congenital disorders of the bones, muscles or joints, disuse or overuse of the bones, muscles or joints caused by illness or disease, diseases, such as bone cancer, Issues of the spine, shoulder or hip, traumatic injuries, such as severe fractures that damage growth plates.
Symptoms
The effects of a short leg depend upon the individual and the extent of discrepancy. The most common manifestation if a lateral deviation of the lumbar spine toward the short side with compensatory curves up the spine that can extend into the neck and even impacts the TMJ. Studies have shown that anterior and posterior curve abnormalities also can result.
Diagnosis
A systematic and well organized approach should be used in the diagnosis of LLD to ensure all relevant factors are considered and no clues are overlooked which could explain the difference. To determine the asymmetry a patient should be evaluated whilst standing and walking. During the process special care should be used to note the extent of pelvic shift from side to side and deviation along the plane of the front or leading leg as well as the traverse deviation of the back leg and abnormal curvature of the spine. Dynamic gait analysis should be conducted during waling where observation of movement on the sagittal, frontal and transverse planes should be noted. Also observe head, neck and shoulder movements for any tilting.
Non Surgical Treatment
Treatment depends on what limb has the deformity and the amount of deformity present. For example, there may be loss of function of the leg or arm. Cosmetic issues may also be a concern for the patient and their family. If there are problems with the arms, the goal is to improve the appearance and function of the arm. Treatment of leg problems try to correct the deformity that may cause arthritis as the child gets older. If the problem is leg length, where the legs are not "equal," the goal is equalization (making the legs the same length). Treatment may include the use of adaptive devices, prosthesis, orthotics or shoe lifts. If the problem is more severe and not treatable with these methods, then surgery may be necessary.

how to increase height naturally after 18
Surgical Treatment
Lengthening is usually done by corticotomy and gradual distraction. This technique can result in lengthenings of 25% or more, but typically lengthening of 15%, or about 6 cm, is recommended. The limits of lengthening depend on patient tolerance, bony consolidation, maintenance of range of motion, and stability of the joints above and below the lengthened limb. Numerous fixation devices are available, such as the ring fixator with fine wires, monolateral fixator with half pins, or a hybrid frame. The choice of fixation device depends on the desired goal. A monolateral device is easier to apply and better tolerated by the patient. The disadvantages of monolateral fixation devices include the limitation of the degree of angular correction that can concurrently be obtained; the cantilever effect on the pins, which may result in angular deformity, especially when lengthening the femur in large patients; and the difficulty in making adjustments without placing new pins. Monolateral fixators appear to have a similar success rate as circular fixators, especially with more modest lengthenings (20%).
In growing children, legs can be made equal or nearly equal in length with a relatively simple surgical procedure. This procedure slows down the growth of the longer leg at one or two growth sites. Your physician can tell you how much equalization can be gained by this procedure. The procedure is performed under X-ray control through very small incisions in the knee area. This procedure will not cause an immediate correction in length. Instead, the limb length discrepancy will gradually decrease as the opposite extremity continues to grow and "catch up." Timing of the procedure is critical. The goal is to reach equal leg length by the time growth normally ends. This is usually in the mid-to-late teenage years. Disadvantages of this option include the possibility of slight over-correction or under-correction of the limb length discrepancy. In addition, the patient's adult height will be less than if the shorter leg had been lengthened. Correction of significant limb length discrepancy by this method may make a patient's body look slightly disproportionate because of the shorter leg. In some cases the longer leg can be shortened, but a major shortening may weaken the muscles of the leg. In the thighbone (femur), a maximum of 3 inches can be shortened. In the shinbone, a maximum of 2 inches can be shortened.
Causes
Limb-length conditions can result from congenital disorders of the bones, muscles or joints, disuse or overuse of the bones, muscles or joints caused by illness or disease, diseases, such as bone cancer, Issues of the spine, shoulder or hip, traumatic injuries, such as severe fractures that damage growth plates.
Symptoms
The effects of a short leg depend upon the individual and the extent of discrepancy. The most common manifestation if a lateral deviation of the lumbar spine toward the short side with compensatory curves up the spine that can extend into the neck and even impacts the TMJ. Studies have shown that anterior and posterior curve abnormalities also can result.
Diagnosis
A systematic and well organized approach should be used in the diagnosis of LLD to ensure all relevant factors are considered and no clues are overlooked which could explain the difference. To determine the asymmetry a patient should be evaluated whilst standing and walking. During the process special care should be used to note the extent of pelvic shift from side to side and deviation along the plane of the front or leading leg as well as the traverse deviation of the back leg and abnormal curvature of the spine. Dynamic gait analysis should be conducted during waling where observation of movement on the sagittal, frontal and transverse planes should be noted. Also observe head, neck and shoulder movements for any tilting.
Non Surgical Treatment
Treatment depends on what limb has the deformity and the amount of deformity present. For example, there may be loss of function of the leg or arm. Cosmetic issues may also be a concern for the patient and their family. If there are problems with the arms, the goal is to improve the appearance and function of the arm. Treatment of leg problems try to correct the deformity that may cause arthritis as the child gets older. If the problem is leg length, where the legs are not "equal," the goal is equalization (making the legs the same length). Treatment may include the use of adaptive devices, prosthesis, orthotics or shoe lifts. If the problem is more severe and not treatable with these methods, then surgery may be necessary.
how to increase height naturally after 18
Surgical Treatment
Lengthening is usually done by corticotomy and gradual distraction. This technique can result in lengthenings of 25% or more, but typically lengthening of 15%, or about 6 cm, is recommended. The limits of lengthening depend on patient tolerance, bony consolidation, maintenance of range of motion, and stability of the joints above and below the lengthened limb. Numerous fixation devices are available, such as the ring fixator with fine wires, monolateral fixator with half pins, or a hybrid frame. The choice of fixation device depends on the desired goal. A monolateral device is easier to apply and better tolerated by the patient. The disadvantages of monolateral fixation devices include the limitation of the degree of angular correction that can concurrently be obtained; the cantilever effect on the pins, which may result in angular deformity, especially when lengthening the femur in large patients; and the difficulty in making adjustments without placing new pins. Monolateral fixators appear to have a similar success rate as circular fixators, especially with more modest lengthenings (20%).
What Causes Mortons Neuroma
Overview
 Morton?s neuroma is inflammation, thickening, or enlargement of the nerve between the bones of the toes (metatarsal bones). The condition is also called intermetatarsal neuroma. The thickening is usually found between bones of the third and fourth toes of the foot, but sometimes it may develop between the second and third toes. It occurs when the medial plantar nerve near the bones of those toes becomes compressed or irritated, possibly because the metatarsal bones press against the nerve in the narrow gap between the toes. If left untreated, Morton?s neuroma can cause a sharp, burning, or shooting pain that often gets worse over time. The pain becomes worse when a person walks or stands on the ball of the foot. Sometimes the pain reaches the toes next to the neuroma and a sensation of tingling or numbness is felt.
Morton?s neuroma is inflammation, thickening, or enlargement of the nerve between the bones of the toes (metatarsal bones). The condition is also called intermetatarsal neuroma. The thickening is usually found between bones of the third and fourth toes of the foot, but sometimes it may develop between the second and third toes. It occurs when the medial plantar nerve near the bones of those toes becomes compressed or irritated, possibly because the metatarsal bones press against the nerve in the narrow gap between the toes. If left untreated, Morton?s neuroma can cause a sharp, burning, or shooting pain that often gets worse over time. The pain becomes worse when a person walks or stands on the ball of the foot. Sometimes the pain reaches the toes next to the neuroma and a sensation of tingling or numbness is felt.
Causes
Morton's neuroma is an inflammation caused by a buildup of fibrous tissue on the outer coating of nerves. This fibrous buildup is a reaction to the irritation resulting from nearby bones and ligaments rubbing against the nerves. Irritation can be caused by Wearing shoes that are too tight. Wearing shoes that place the foot in an awkward position, such as high heels. A foot that is mechanically unstable. Repetitive trauma to the foot such as from sports activities like tennis, basketball, and running. Trauma to the foot caused by an injury such as a sprain or fracture. It is unusual for more than one Morton's neuroma to occur on one foot at the same time. It is rare for Morton's neuroma to occur on both feet at the same time.
Symptoms
Often, no outward signs (such as a lump or unusual swelling) appear from the condition. Neuroma pain is most often described as a burning discomfort in the forefoot. Aching or sudden shooting pain in the forefoot is also common. All running sports, especially distance running can leave an athlete vulnerable to Morton?s Neuroma, which may appear or flare up in the middle of a run or at the end. The sufferer often has the desire to remove his shoe and rub the afflicted foot. Should the Neuroma be of sufficient size, or if footwear is particularly tight or uncomfortable, the painful condition may be present during normal walking. Numbness in the foot may precede or accompany Neuroma pain.
Diagnosis
Podiatrists conduct a physical examination and may order imaging tests, such as x-ray or MRI scan to diagnose Morton's neuroma. Conservative treatment options include custom-fitted orthotics, medication, and/or alcohol injections designed to harden the nerve. However, most patients with Morton's neuroma need minor surgery.
Non Surgical Treatment
If you have Morton's neuroma, shoes with a wider toe area may be recommended. You can also take painkillers to help ease the pain. Steroid injections may also be given to treat the affected nerve. If these treatments don't work, surgery may be needed. This involves removing the thickened tissue around the nerve (and sometimes the nerve itself) to release the pressure.
Surgical Treatment
Surgery to excise the neuroma is usually performed under general anaesthetic in a day surgery facility. After surgery you will have to keep your foot dry for two weeks. Generally neuroma surgery allows for early weight bearing and protection in some type of post op shoe gear. Some neuromas may reoccur, but this is rare. Most studies on patient satisfaction after neuroma surgery show approximately 90% reduction of pain and about 85% of all patients rated the overall satisfaction with the results as excellent or good.
Prevention
Always warm-up thoroughly before vigorous athletics. Avoid activities that cause pain. Stretch and strengthen the feet through gradual exercise.
Morton?s neuroma is inflammation, thickening, or enlargement of the nerve between the bones of the toes (metatarsal bones). The condition is also called intermetatarsal neuroma. The thickening is usually found between bones of the third and fourth toes of the foot, but sometimes it may develop between the second and third toes. It occurs when the medial plantar nerve near the bones of those toes becomes compressed or irritated, possibly because the metatarsal bones press against the nerve in the narrow gap between the toes. If left untreated, Morton?s neuroma can cause a sharp, burning, or shooting pain that often gets worse over time. The pain becomes worse when a person walks or stands on the ball of the foot. Sometimes the pain reaches the toes next to the neuroma and a sensation of tingling or numbness is felt.Causes
Morton's neuroma is an inflammation caused by a buildup of fibrous tissue on the outer coating of nerves. This fibrous buildup is a reaction to the irritation resulting from nearby bones and ligaments rubbing against the nerves. Irritation can be caused by Wearing shoes that are too tight. Wearing shoes that place the foot in an awkward position, such as high heels. A foot that is mechanically unstable. Repetitive trauma to the foot such as from sports activities like tennis, basketball, and running. Trauma to the foot caused by an injury such as a sprain or fracture. It is unusual for more than one Morton's neuroma to occur on one foot at the same time. It is rare for Morton's neuroma to occur on both feet at the same time.
Symptoms
Often, no outward signs (such as a lump or unusual swelling) appear from the condition. Neuroma pain is most often described as a burning discomfort in the forefoot. Aching or sudden shooting pain in the forefoot is also common. All running sports, especially distance running can leave an athlete vulnerable to Morton?s Neuroma, which may appear or flare up in the middle of a run or at the end. The sufferer often has the desire to remove his shoe and rub the afflicted foot. Should the Neuroma be of sufficient size, or if footwear is particularly tight or uncomfortable, the painful condition may be present during normal walking. Numbness in the foot may precede or accompany Neuroma pain.
Diagnosis
Podiatrists conduct a physical examination and may order imaging tests, such as x-ray or MRI scan to diagnose Morton's neuroma. Conservative treatment options include custom-fitted orthotics, medication, and/or alcohol injections designed to harden the nerve. However, most patients with Morton's neuroma need minor surgery.
Non Surgical Treatment
If you have Morton's neuroma, shoes with a wider toe area may be recommended. You can also take painkillers to help ease the pain. Steroid injections may also be given to treat the affected nerve. If these treatments don't work, surgery may be needed. This involves removing the thickened tissue around the nerve (and sometimes the nerve itself) to release the pressure.
Surgical Treatment
Surgery to excise the neuroma is usually performed under general anaesthetic in a day surgery facility. After surgery you will have to keep your foot dry for two weeks. Generally neuroma surgery allows for early weight bearing and protection in some type of post op shoe gear. Some neuromas may reoccur, but this is rare. Most studies on patient satisfaction after neuroma surgery show approximately 90% reduction of pain and about 85% of all patients rated the overall satisfaction with the results as excellent or good.
Prevention
Always warm-up thoroughly before vigorous athletics. Avoid activities that cause pain. Stretch and strengthen the feet through gradual exercise.
The Solution To Leg Length Discrepancy Are Shoe Lifts
There are not one but two different types of leg length discrepancies, congenital and acquired. Congenital means that you are born with it. One leg is anatomically shorter compared to the other. As a result of developmental phases of aging, the human brain senses the walking pattern and recognizes some difference. The body usually adapts by tilting one shoulder to the "short" side. A difference of less than a quarter inch is not grossly uncommon, demand Shoe Lifts to compensate and generally won't have a serious effect over a lifetime.

Leg length inequality goes mainly undiagnosed on a daily basis, however this issue is simply corrected, and can eradicate quite a few incidents of back discomfort.
Therapy for leg length inequality commonly involves Shoe Lifts. Many are low-priced, often costing below twenty dollars, in comparison to a custom orthotic of $200 plus. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position.
Low back pain is easily the most prevalent ailment affecting people today. Over 80 million men and women are affected by back pain at some stage in their life. It's a problem which costs employers millions year after year due to lost time and production. New and more effective treatment methods are continually sought after in the hope of lowering economic influence this condition causes.

Men and women from all corners of the world suffer the pain of foot ache as a result of leg length discrepancy. In these cases Shoe Lifts might be of immense help. The lifts are capable of alleviating any discomfort in the feet. Shoe Lifts are recommended by countless skilled orthopaedic orthopedists.
In order to support the human body in a well balanced manner, your feet have a very important part to play. Despite that, it can be the most overlooked zone in the human body. Many people have flat-feet which means there may be unequal force exerted on the feet. This causes other areas of the body like knees, ankles and backs to be affected too. Shoe Lifts make sure that the right posture and balance are restored.
Leg length inequality goes mainly undiagnosed on a daily basis, however this issue is simply corrected, and can eradicate quite a few incidents of back discomfort.
Therapy for leg length inequality commonly involves Shoe Lifts. Many are low-priced, often costing below twenty dollars, in comparison to a custom orthotic of $200 plus. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position.
Low back pain is easily the most prevalent ailment affecting people today. Over 80 million men and women are affected by back pain at some stage in their life. It's a problem which costs employers millions year after year due to lost time and production. New and more effective treatment methods are continually sought after in the hope of lowering economic influence this condition causes.
Men and women from all corners of the world suffer the pain of foot ache as a result of leg length discrepancy. In these cases Shoe Lifts might be of immense help. The lifts are capable of alleviating any discomfort in the feet. Shoe Lifts are recommended by countless skilled orthopaedic orthopedists.
In order to support the human body in a well balanced manner, your feet have a very important part to play. Despite that, it can be the most overlooked zone in the human body. Many people have flat-feet which means there may be unequal force exerted on the feet. This causes other areas of the body like knees, ankles and backs to be affected too. Shoe Lifts make sure that the right posture and balance are restored.
What Is Posterior Calcaneal Spur
Overview
Approximately 10 per cent of the population may have heel spurs without any heel pain. Whilst recent research has raised the question of whether or not heel spurs are the result of the body trying to increase its base of support, heel spurs are still considered to be the result from strain on the muscles of the foot (in particular the plantar fascia). This may result from a biomechanical imbalance, such as over pronation.
Causes
A heel spur is caused by chronic plantar fasciitis. Your plantar fascia is a thick fibrous band of connective tissue originating on the bottom surface of the calcaneus (heel bone) and extending along the sole of the foot towards the toes.Your plantar fascia acts as a passive limitation to the over flattening of you arch. When your plantar fascia develops micro tears or becomes inflamed it is known as plantar fasciitis. When plantar fasciitis healing is delayed or injury persists, your body repairs the weak and injured soft tissue with bone. Usually your injured fascia will be healed via fibroblastic activity. They'll operate for at least six weeks. If your injury persists beyond this time, osteoblasts are recruited to the area. Osteoblasts form bone and the end result is bone (or calcification) within the plantar fascia or at the calcaneal insertion. These bone formations are known as heel spurs. This scenario is most common in the traction type injury. The additional bone growth is known as a heel spur or calcaneal spur.

Symptoms
Most heel spurs cause no symptoms and may go undetected for years. If they cause no pain or discomfort, they require no treatment. Occasionally, a bone spur will break off from the larger bone, becoming a ?loose body?, floating in a joint or embedding itself in the lining of the joint. This can cause pain and intermittent locking of the joint. In the case of heel spurs, sharp pain and discomfort is felt on the bottom of the foot or heel.
Diagnosis
A Diagnosis of Heel Spur Syndrome is a very common reason for having heel pain. Heel pain may be due to other types of conditions such as tendonitis, Haglund's Deformity, Stress Fracture, Tarsal Tunnel Syndrome, or low back problems. A more common condition in children is Sever's Disease. The diagnosis is usually made with a combination of x-ray examination and symptoms.
Non Surgical Treatment
Bone spurs rarely require treatment unless they are causing frequent pain or damaging other tissues. Because heel spurs and plantar fasciitis are so closely related, they are usually treated the same way. Symptomatic treatment involves rest, especially from the activity that is contributing to the condition and making symptoms worse (although this may not be easy to discover, as problems can manifest several hours or days after the harmful activity has occurred). If you identify the offending activity, ice is recommended immediately following it. Stretching of the calf muscles after a short warm up is also a good idea and can be helpful. Stretching exercises that gently lengthen the calm muscle will relax the tissue surrounding the heel and should be done several times a day, especially in the morning and after prolonged sitting.
Surgical Treatment
Sometimes bone spurs can be surgically removed or an operation to loosen the fascia, called a plantar fascia release can be performed. This surgery is about 80 percent effective in the small group of individuals who do not have relief with conservative treatment, but symptoms may return if preventative measures (wearing proper footwear, shoe inserts, stretching, etc) are not maintained.