Tips To Treat Posterior Calcaneal Spur
Overview
A heel spur is a bony growth at the underside of the heel bone. The underlying cause of heel spurs is a common condition called ?Plantar Fasciitis?. This is Latin for inflammation of the plantar fascia. This tendon forms the arch of the foot, starting at the heel and running to the ball of the foot. Plantar Fasciitis is a persistent and painful condition. Interestingly, in some people a heel spur has been present for a long time, but no pain is felt for years until one day the pain suddenly appears ?out of nothing?.
Causes
When a bone is subjected to pressure, rubbing, or other stress over long periods, it tries to repair itself by building extra bone. This extra bone is what is referred to as a ?spur?. Many form as part of the aging process when cartilage breaks down in the joints.

Symptoms
Symptoms may be similar to those of plantar fasciitis and include pain and tenderness at the base of the heel, pain on weight bearing and in severe cases difficulty walking. The main diagnosis of a heel spur is made by X-ray where a bony growth on the heel can be seen. A heel spur can occur without any symptoms at all and the athlete would never know they have the bony growth on the heel. Likewise, Plantar fasciitis can occur without the bone growth present.
Diagnosis
A thorough medical history and physical exam by a physician is always necessary for the proper diagnosis of heel spurs and other foot conditions. X rays of the heel area are helpful, as excess bone production will be visible.
Non Surgical Treatment
Conventional treatment for heel spurs typically includes rest, stretching exercises, icing and anti-inflammatory medications. Many people find it difficult to go through the day without some sort of routine activity or exercise, and this prolongs the heel spur and forces people to rely on anti-inflammatory medications for a longer period of time. This can be detrimental due to the many side effects of these medications, including gastrointestinal problems like leaky gut, bleeding and ulcer symptoms.
Surgical Treatment
Though conservative treatments for heel spurs work most of the time, there are some cases where we need to take your treatment to the next level. Luckily, with today?s technologies, you can still often avoid surgery. Some of the advanced technologies to treat a Heel Spur are Platelet Rich Plasma Therapy. Platelet Rich Plasma Therapy (also known as PRP) is one of several regenerative medicine techniques that University Foot and Ankle Institute has helped bring to foot and ankle care. This amazing in-office procedure allows the growth factors in the blood to be used to actually begin the healing process again long after your body has given up on healing the area. Heel Pain Shockwave Therapy. Shockwave therapy is a non-invasive procedure done in the office that allows for new blood to get to the region of fascia damage and help with healing. Results have been excellent with more than 70 percent of patients getting relief with only one treatment. Topaz for Heal Spurs and pain. Another minimally invasive technology technique is called Coblation Surgery using a Topaz probe. This minimally invasive procedure involves controlled heating of multiple tiny needles that are inserted through the skin and into the plantar fascia. This process, like PRP and Shockwave therapy, irritates the fascia enough to turn a chronic problem back into an acute problem, greatly increasing the chances of healing. Heel Spur Surgery. Endoscopic Plantar Fasciotomy is one surgical procedure that we consider to release the tight fascia. University Foot and Ankle Institute has perfected an endoscopic (camera guided) approach for fascia release to allow rapid healing and limited downtime with minimal pain.
Cure For Bursitis Of The Feet
Overview
Heel bursitis is a common foot pain in athletes, and is often mistaken for Achilles tendinitis, although it can also occur together with Achilles tendinitis. Heel bursitis occurs when small cushions in the heel called bursas become inflamed and swell with fluid irritating surrounding tissue and pressing on nerves. Other names given to heel bursitis are Achilles bursitis and Retrocalcaneal bursitis.
Causes
Inflammation of the bursa causes synovial cells to multiply and thereby increases collagen formation and fluid production. A more permeable capillary membrane allows entrance of high protein fluid. The bursal lining may be replaced by granulation tissue followed by fibrous tissue. The bursa becomes filled with fluid, which is often rich in fibrin, and the fluid can become hemorrhagic. One study suggests that this process may be mediated by cytokines, metalloproteases, and cyclooxygenases.
Symptoms
You might have Retrocalcaneal Bursitis if you notice any of the following symptoms. You have pain or tenderness at the back of the heel where the Achille's tendon attaches. Have swelling near the attachment of the tendon to the heel bone. You have noticed a slowly growing bump on the back of the heel. The back of the heel turns red after getting rubbed in shoes. The back of the heel hurts worse when you run, walk up hill or wear high heels.
Diagnosis
Before making a diagnosis of retrocalcaneal bursitis, a doctor must rule out other possible problems, such as arthritis, a fracture or tumor. A doctor also will try to determine if the Achilles tendon itself is a source of pain. To make a diagnosis, a doctor will use some or all of the diagnostic tools below Patient interview. A doctor will ask a patient about medical history, and to describe the onset of his or her symptoms, the pattern of pain and swelling, and how symptoms affect lifestyle. For example, doctors may ask patients what types of shoes they wear and what they do for exercise. A patient's reported symptoms are important to diagnosis and treatment. The doctor will also ask what home treatments have helped the condition. Physical exam. A doctor will examine the patient's foot, noting swelling, tenderness and pain points, and range of motion. The doctor also may ask the patient to point and flex the feet and stand on his or her toes.
Non Surgical Treatment
Caregivers may give you special shoe inserts with a cutout around the tender area. You may also be told to wear shoes with a reinforced heel counter. This will give better heel control. You may need other shoe inserts (wedges) to raise your heel so it does not press against the back of the shoe. You may also wear shoes that are open in the back, such as sandals that have no strap across the heel. You may use ibuprofen (eye-bu-PROH-fen) and acetaminophen (a-seet-a-MIN-oh-fen) medicine for your pain. These may be bought over-the-counter at drug or grocery stores. Do not take ibuprofen if you are allergic to aspirin. You may be given shots of medicine called steroids (STER-oids) to decrease inflammation. Caregivers may add local anesthesia (an-es-THEE-zah) to the steroids. This medicine helps decrease bursitis pain. Because these shots decrease swelling and pain, you may feel like your ankle is healed and that you can return to heavy exercise. It is important to not exercise until your caregiver says it is OK. You could make the bursitis worse if you exercise too soon. You may need surgery to remove the bursa or part of your ankle bone. Surgery is usually not necessary unless the bursitis is very bad and does not heal with other treatments. Your caregiver may want you to go to physical (FIZ-i-kal) therapy (THER-ah-pee). Physical therapists may use ultrasound to increase blood flow to the injured area. Caregivers may use massage to stretch the tissue and bring heat to the injury to increase blood flow. These and other treatments may help the bursitis heal faster. Exercises to stretch your Achilles tendon and make it stronger will be started after the bursitis has healed. You may gradually increase the amount of weight you put on your foot when caregivers say it is OK. You may be told to stop exercising if you feel any pain.
Prevention
People can lower the risk of bursitis by gradually strengthening and stretching the muscles around the joints and taking regular breaks from repetitive motion that might irritate bursae. Prolonged time resting on the elbows or kneeling should be avoided, if it cannot be avoided, wearing cushioned elbow and knee pads can help protect the bursae. Comfortable, supportive, low-heeled shoes can help prevent bursitis in the foot.
Heel bursitis is a common foot pain in athletes, and is often mistaken for Achilles tendinitis, although it can also occur together with Achilles tendinitis. Heel bursitis occurs when small cushions in the heel called bursas become inflamed and swell with fluid irritating surrounding tissue and pressing on nerves. Other names given to heel bursitis are Achilles bursitis and Retrocalcaneal bursitis.
Causes
Inflammation of the bursa causes synovial cells to multiply and thereby increases collagen formation and fluid production. A more permeable capillary membrane allows entrance of high protein fluid. The bursal lining may be replaced by granulation tissue followed by fibrous tissue. The bursa becomes filled with fluid, which is often rich in fibrin, and the fluid can become hemorrhagic. One study suggests that this process may be mediated by cytokines, metalloproteases, and cyclooxygenases.
Symptoms
You might have Retrocalcaneal Bursitis if you notice any of the following symptoms. You have pain or tenderness at the back of the heel where the Achille's tendon attaches. Have swelling near the attachment of the tendon to the heel bone. You have noticed a slowly growing bump on the back of the heel. The back of the heel turns red after getting rubbed in shoes. The back of the heel hurts worse when you run, walk up hill or wear high heels.
Diagnosis
Before making a diagnosis of retrocalcaneal bursitis, a doctor must rule out other possible problems, such as arthritis, a fracture or tumor. A doctor also will try to determine if the Achilles tendon itself is a source of pain. To make a diagnosis, a doctor will use some or all of the diagnostic tools below Patient interview. A doctor will ask a patient about medical history, and to describe the onset of his or her symptoms, the pattern of pain and swelling, and how symptoms affect lifestyle. For example, doctors may ask patients what types of shoes they wear and what they do for exercise. A patient's reported symptoms are important to diagnosis and treatment. The doctor will also ask what home treatments have helped the condition. Physical exam. A doctor will examine the patient's foot, noting swelling, tenderness and pain points, and range of motion. The doctor also may ask the patient to point and flex the feet and stand on his or her toes.
Non Surgical Treatment
Caregivers may give you special shoe inserts with a cutout around the tender area. You may also be told to wear shoes with a reinforced heel counter. This will give better heel control. You may need other shoe inserts (wedges) to raise your heel so it does not press against the back of the shoe. You may also wear shoes that are open in the back, such as sandals that have no strap across the heel. You may use ibuprofen (eye-bu-PROH-fen) and acetaminophen (a-seet-a-MIN-oh-fen) medicine for your pain. These may be bought over-the-counter at drug or grocery stores. Do not take ibuprofen if you are allergic to aspirin. You may be given shots of medicine called steroids (STER-oids) to decrease inflammation. Caregivers may add local anesthesia (an-es-THEE-zah) to the steroids. This medicine helps decrease bursitis pain. Because these shots decrease swelling and pain, you may feel like your ankle is healed and that you can return to heavy exercise. It is important to not exercise until your caregiver says it is OK. You could make the bursitis worse if you exercise too soon. You may need surgery to remove the bursa or part of your ankle bone. Surgery is usually not necessary unless the bursitis is very bad and does not heal with other treatments. Your caregiver may want you to go to physical (FIZ-i-kal) therapy (THER-ah-pee). Physical therapists may use ultrasound to increase blood flow to the injured area. Caregivers may use massage to stretch the tissue and bring heat to the injury to increase blood flow. These and other treatments may help the bursitis heal faster. Exercises to stretch your Achilles tendon and make it stronger will be started after the bursitis has healed. You may gradually increase the amount of weight you put on your foot when caregivers say it is OK. You may be told to stop exercising if you feel any pain.
Prevention
People can lower the risk of bursitis by gradually strengthening and stretching the muscles around the joints and taking regular breaks from repetitive motion that might irritate bursae. Prolonged time resting on the elbows or kneeling should be avoided, if it cannot be avoided, wearing cushioned elbow and knee pads can help protect the bursae. Comfortable, supportive, low-heeled shoes can help prevent bursitis in the foot.
Is A Hammer Toe Uncomfortable
 Overview
Overview
A Hammer toes is commonly mistaken hammertoe as any type of toe deformity. The terms claw toe, or mallet toe, although technically different than a hammer toe, are commonly referred as such. The toe may be flexible with movement at the joints, or it may be rigid, especially if it has been present for a long time. With a true hammertoe the deformity exists at the proximal interphalangeal joint only.
Causes
A hammer toe develops because of an abnormal balance of the muscles in the toes. This abnormal balance causes increased pressures on the tendons and joints of the toe, leading to its contracture. Heredity and trauma can also lead to the formation of a hammer toe. Arthritis is another factor, because the balance around the toe in people with arthritis is disrupted. Wearing shoes that are too tight and cause the toes to squeeze can also cause a hammer toe to form.
 Symptoms
Symptoms
The symptoms of hammertoe include a curling toe, pain or discomfort in the toes and ball of the foot or the front of the leg, especially when toes are stretched downward. Thickening of the skin above or below the affected toe with the formation of corns or calluses. Difficulty finding shoes that fit well. In its early stages, hammertoe is not obvious. Frequently, hammertoe does not cause any symptoms except for the claw-like toe shape.
Diagnosis
Most health care professionals can diagnose hammertoe simply by examining your toes and feet. X-rays of the feet are not needed to diagnose hammertoe, but they may be useful to look for signs of some types of arthritis (such as rheumatoid arthritis) or other disorders that can cause hammertoe. If the deformed toe is very painful, your doctor may recommend that you have a fluid sample withdrawn from the joint with a needle so the fluid can be checked for signs of infection or gout (arthritis from crystal deposits).
Non Surgical Treatment
Your doctor may prescribe some toe exercises that you can do at home to stretch and strengthen the muscles. For example, you can gently stretch the toes manually. You can use your toes to pick things up off the floor. While you watch television or read, you can put a towel flat under your feet and use your toes to crumple it. Finally, your doctor may recommend that you use commercially available straps, cushions or nonmedicated corn pads to relieve symptoms. If you have diabetes, poor circulation or a lack of feeling in your feet, talk to your doctor before attempting any self-treatment.
Surgical Treatment
Surgery to correct for a hammertoe may be performed as a day procedure. There are several different types of procedures that can be used depending on the foot structure and if the deformity is flexible or rigid.
Non Surgical Treatment For Hammer Toes
 Overview
Overview
Hammer toes a bending and hardening of the joints of the second, third, fourth, or fifth toes. If you look down at your feet and you can?t see the tips of the toenails, you might suffer from hammertoe. Early signs of hammertoe are a bend in the joint of any toe except the big toe. The bend in the joint causes the top of the toe to appear to curl under as if it?s ?hammering? into the floor.
Causes
Many people develop hammertoe because they wear shoes that are too tight. Shoes with narrow toe boxes squeeze the toes together, forcing some to bend. This causes the toe muscles to contract. If the toes are forced into this cramped position too often, the muscles may permanently tighten, preventing the toes from extending. Chronic hammertoe can also hammertoe cause the long bones that connect the toes to the foot, called metatarsals, to move out of position. The misaligned metatarsal bones may pinch a nerve running between them, which can cause a type of nerve irritation called a neuroma.
 Symptoms
Symptoms
The most obvious symptom of hammertoe is the bent, hammer-like or claw-like appearance of one or more of your toes. Typically, the proximal joint of a toe will be bending upward and the distal joint will be bending downward. In some cases, both joints may bend downward, causing the toes to curl under the foot. In the variation of mallet toe, only the distal joint bends downward. Other symptoms may include Pain and stiffness during movement of the toe, Painful corns on the tops of the toe or toes from rubbing against the top of the shoe's toe box, Painful calluses on the bottoms of the toe or toes, Pain on the bottom of the ball of the foot, Redness and swelling at the joints. If you have any of these symptoms, especially the hammer shape, pain or stiffness in a toe or toes, you should consider consulting your physician. Even if you're not significantly bothered by some of these symptoms, the severity of a hammertoe can become worse over time and should be treated as soon as possible. Up to a point hammertoes can be treated without surgery and should be taken care of before they pass that point. After that, surgery may be the only solution.
Diagnosis
Your healthcare provider will examine your foot, checking for redness, swelling, corns, and calluses. Your provider will also measure the flexibility of your toes and test how much feeling you have in your toes. You may have blood tests to check for arthritis, diabetes, and infection.
Non Surgical Treatment
Inserts in your shoes can be used to help relieve pressure on the toes from the deformity. Splints/Straps. These can be used to help re-align and stretch your toes and correct the muscle imbalance and tendon shortening. One of the most common types are toe stretchers like the yogatoe. Chiropody. A chiropodist can remove calluses or corns, areas of hard skin that have formed to make the foot more comfortable.Steroid injections can help to reduce pain and inflammation.
Surgical Treatment
Surgery is used when other types of treatment fail to relieve symptoms or for advanced cases of hammertoe. There are several types of surgeries to treat hammertoe. A small piece of bone may be removed from the joint (arthroplasty). The toe joint may be fused to straighten it (arthrodesis). Surgical hardware, such as a pin, may be used to hold the bones in place while they heal. Other types of surgery involve removing skin (wedging) or correcting muscles and tendons to balance the joint.
 Prevention
Prevention
Prevention of a hammer toe can be difficult as symptoms do not usually start until the problem is well established. Wearing shoes that have extra room in the toes may help the problem or slow down its development.
Will Over-Pronation Need An Operation
Overview
Over-pronation is very common and affects millions of people. To better understand this condition, we'll take a closer look at the 3 most common foot types. An estimated 70% of the population has fallen arches (or a low arch). Only 20% has a normal arch. And 10% have abnormal feet, in other words they either have flat feet or the opposite a high arched foot.
Causes
Over-pronation may happen because the tissue that attaches to your foot bones is loose. You may be born with this problem or it may result from injuries or overuse, like from too much running.
Symptoms
Over-pronation is a condition where the arch flattens out which makes the feet roll inward while walking. This condition is also known as flat feet. It imposes extreme additional stresses on the plantar fascia, a fibrous band of tissue which connects the heel to the forefoot. Over-pronation makes walking a painful experience because of the additional strain on the calves, heel and/or back. Treatment for over-pronation involves the use of specially-made orthotics which offers arch support and medial rear foot posting as corrective measures.
Diagnosis
The best way to discover whether you have a normal gait, or if you overpronate, is to visit a specialty run shop, an exercise physiologist, a podiatrist or a physical therapist who specializes in working with athletes. A professional can analyze your gait, by watching you either walk or run, preferably on a treadmill. Some facilities can videotape your gait, then analyze the movement of your feet in slow-motion. Another (and less costly) way is to look at the bottom of an older pair of run shoes. Check the wear pattern. A person with a normal gait will generally see wear evenly across the heel and front of the shoe. A person who overpronates will likely see more wear on the OUTside of the heel and more wear on the INside of the forefoot (at the ball). A person who supinates will see wear all along the outer edges of the shoe. You can also learn about your gait by looking at your arches. Look at the shape your wet feet leave on a piece of paper or a flat walking surface.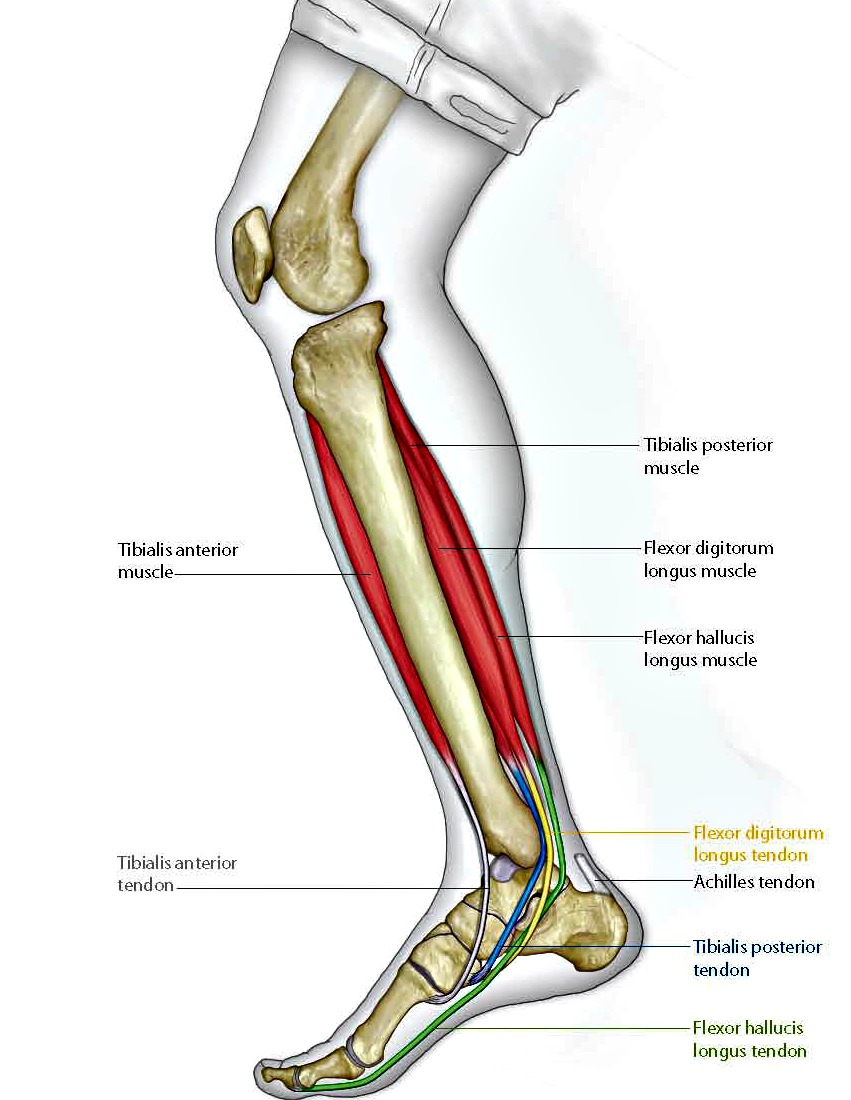
Non Surgical Treatment
Over-Pronation can be treated conservatively (non-surgical treatments) with over-the-counter orthotics. These orthotics should be designed with appropriate arch support and medial rearfoot posting to prevent the over-pronation. Footwear should also be examined to ensure there is a proper fit. Footwear with a firm heel counter is often recommended for extra support and stability. Improperly fitting footwear can lead to additional foot problems.
Surgical Treatment
Depending on the severity of your condition, your surgeon may recommend one or more treatment options. Ultimately, however, it's YOUR decision as to which makes the most sense to you. There are many resources available online and elsewhere for you to research the various options and make an informed decision.
Over-pronation is very common and affects millions of people. To better understand this condition, we'll take a closer look at the 3 most common foot types. An estimated 70% of the population has fallen arches (or a low arch). Only 20% has a normal arch. And 10% have abnormal feet, in other words they either have flat feet or the opposite a high arched foot.
Causes
Over-pronation may happen because the tissue that attaches to your foot bones is loose. You may be born with this problem or it may result from injuries or overuse, like from too much running.
Symptoms
Over-pronation is a condition where the arch flattens out which makes the feet roll inward while walking. This condition is also known as flat feet. It imposes extreme additional stresses on the plantar fascia, a fibrous band of tissue which connects the heel to the forefoot. Over-pronation makes walking a painful experience because of the additional strain on the calves, heel and/or back. Treatment for over-pronation involves the use of specially-made orthotics which offers arch support and medial rear foot posting as corrective measures.
Diagnosis
The best way to discover whether you have a normal gait, or if you overpronate, is to visit a specialty run shop, an exercise physiologist, a podiatrist or a physical therapist who specializes in working with athletes. A professional can analyze your gait, by watching you either walk or run, preferably on a treadmill. Some facilities can videotape your gait, then analyze the movement of your feet in slow-motion. Another (and less costly) way is to look at the bottom of an older pair of run shoes. Check the wear pattern. A person with a normal gait will generally see wear evenly across the heel and front of the shoe. A person who overpronates will likely see more wear on the OUTside of the heel and more wear on the INside of the forefoot (at the ball). A person who supinates will see wear all along the outer edges of the shoe. You can also learn about your gait by looking at your arches. Look at the shape your wet feet leave on a piece of paper or a flat walking surface.
Non Surgical Treatment
Over-Pronation can be treated conservatively (non-surgical treatments) with over-the-counter orthotics. These orthotics should be designed with appropriate arch support and medial rearfoot posting to prevent the over-pronation. Footwear should also be examined to ensure there is a proper fit. Footwear with a firm heel counter is often recommended for extra support and stability. Improperly fitting footwear can lead to additional foot problems.
Surgical Treatment
Depending on the severity of your condition, your surgeon may recommend one or more treatment options. Ultimately, however, it's YOUR decision as to which makes the most sense to you. There are many resources available online and elsewhere for you to research the various options and make an informed decision.
Severs Disease Physical Therapy
Overview
If your child is experiencing activity related pain just below the kneecap, at the top of the shinbone, or in their heel or hip then the chances are they are suffering from Osgood Schlatter, Severs disease or Ischial Apophysitis respectively. Today, thousands of children are diagnosed with one of these conditions every year. Many others are never diagnosed and the discomfort is often dismissed as 'growing pains'
Causes
Your child is most at risk for this condition when he or she is in the early part of the growth spurt in early puberty. Sever's disease is most common in physically active girls 8 years to 10 years of age and in physically active boys 10 years to 12 years of age. Soccer players and gymnasts often get Sever's disease, but children who do any running or jumping activity may also be at an increased risk. Sever's disease rarely occurs in older teenagers because the back of the heel has typically finished growing by 15 years of age.
Symptoms
The most obvious sign of Sever's disease is pain or tenderness in one or both heels, usually at the back. The pain also might extend to the sides and bottom of the heel, ending near the arch of the foot. A child also may have these related problems, swelling and redness in the heel, difficulty walking, discomfort or stiffness in the feet upon awaking, discomfort when the heel is squeezed on both sides, an unusual walk, such as walking with a limp or on tiptoes to avoid putting pressure on the heel. Symptoms are usually worse during or after activity and get better with rest.
Diagnosis
A physical exam of the heel will show tenderness over the back of the heel but not in the Achilles tendon or plantar fascia. There may be tightness in the calf muscle, which contributes to tension on the heel. The tendons in the heel get stretched more in patients with flat feet. There is greater impact force on the heels of athletes with a high-arched, rigid foot. The doctor may order an x-ray because x-rays can confirm how mature the growth center is and if there are other sources of heel pain, such as a stress fracture or bone cyst. However, x-rays are not necessary to diagnose Sever?s disease, and it is not possible to make the diagnosis based on the x-ray alone.
Non Surgical Treatment
First, your child should cut down or stop any activity that causes heel pain. Apply ice to the injured heel for 20 minutes 3 times a day. If your child has a high arch, flat feet or bowed legs, your doctor may recommend orthotics, arch supports or heel cups. Your child should never go barefoot. If your child has severe heel pain, medicines such as acetaminophen (one brand name: Tylenol) or ibuprofen (some brand names. Advil, Motrin, Nuprin) may help.
Prevention
The best way to prevent Sever's disease is to make sure that your child wears shoes that fit properly. The heel portion of the shoe should not be too tight, and there should be good padding in the heel. It may help to put extra heel pads in your child's shoes. Some children simply get too much physical activity. For example, they may play on too many teams or practice for too long. Their heel pain is a message to slow down.
If your child is experiencing activity related pain just below the kneecap, at the top of the shinbone, or in their heel or hip then the chances are they are suffering from Osgood Schlatter, Severs disease or Ischial Apophysitis respectively. Today, thousands of children are diagnosed with one of these conditions every year. Many others are never diagnosed and the discomfort is often dismissed as 'growing pains'
Causes
Your child is most at risk for this condition when he or she is in the early part of the growth spurt in early puberty. Sever's disease is most common in physically active girls 8 years to 10 years of age and in physically active boys 10 years to 12 years of age. Soccer players and gymnasts often get Sever's disease, but children who do any running or jumping activity may also be at an increased risk. Sever's disease rarely occurs in older teenagers because the back of the heel has typically finished growing by 15 years of age.
Symptoms
The most obvious sign of Sever's disease is pain or tenderness in one or both heels, usually at the back. The pain also might extend to the sides and bottom of the heel, ending near the arch of the foot. A child also may have these related problems, swelling and redness in the heel, difficulty walking, discomfort or stiffness in the feet upon awaking, discomfort when the heel is squeezed on both sides, an unusual walk, such as walking with a limp or on tiptoes to avoid putting pressure on the heel. Symptoms are usually worse during or after activity and get better with rest.
Diagnosis
A physical exam of the heel will show tenderness over the back of the heel but not in the Achilles tendon or plantar fascia. There may be tightness in the calf muscle, which contributes to tension on the heel. The tendons in the heel get stretched more in patients with flat feet. There is greater impact force on the heels of athletes with a high-arched, rigid foot. The doctor may order an x-ray because x-rays can confirm how mature the growth center is and if there are other sources of heel pain, such as a stress fracture or bone cyst. However, x-rays are not necessary to diagnose Sever?s disease, and it is not possible to make the diagnosis based on the x-ray alone.
Non Surgical Treatment
First, your child should cut down or stop any activity that causes heel pain. Apply ice to the injured heel for 20 minutes 3 times a day. If your child has a high arch, flat feet or bowed legs, your doctor may recommend orthotics, arch supports or heel cups. Your child should never go barefoot. If your child has severe heel pain, medicines such as acetaminophen (one brand name: Tylenol) or ibuprofen (some brand names. Advil, Motrin, Nuprin) may help.
Prevention
The best way to prevent Sever's disease is to make sure that your child wears shoes that fit properly. The heel portion of the shoe should not be too tight, and there should be good padding in the heel. It may help to put extra heel pads in your child's shoes. Some children simply get too much physical activity. For example, they may play on too many teams or practice for too long. Their heel pain is a message to slow down.
The Cause And Treatment Of Posterior Tibial Tendon Dysfunction (PTTD)
Overview
Over 60 Million Americans suffer from Adult Acquired Flatfoot (AAF), otherwise known as Posterior Tibial Tendon Dysfunction or PTTD. This condition generally occurs in adults from 40-65 years of age, and it usually only occurs in one foot, not both. The Posterior Tibial (PT) Tendon courses along the inside part of the ankle and underneath the arch of the foot. It is the major supporting structure for the arch. Over time, the tendon becomes diseased, from overuse, and starts to lose it's strength. As a result, the arch begins to collapse, placing further strain on the PT Tendon, leading to further decrease in tendon strength, which causes further collapse of the arch. This is described as a progressive deformity because it will generally get worse over time. 
Causes
Posterior tibial tendon dysfunction is the most common cause of acquired adult flatfoot. Sometimes this can be a result of specific trauma, but usually the tendon becomes injured from wear and tear over time. This is more prevalent in individuals with an inherited flat foot but excessive weight, age, and level of activity are also contributing factors.
Symptoms
Symptoms of pain may have developed gradually as result of overuse or they may be traced to one minor injury. Typically, the pain localizes to the inside (medial) aspect of the ankle, under the medial malleolus. However, some patients will also experience pain over the outside (lateral) aspect of the hindfoot because of the displacement of the calcaneus impinging with the lateral malleolus. This usually occurs later in the course of the condition. Patients may walk with a limp or in advanced cases be disabled due to pain. They may also have noticed worsening of their flatfoot deformity.
Diagnosis
First, both feet should be examined with the patient standing and the entire lower extremity visible. The foot should be inspected from above as well as from behind the patient, as valgus angulation of the hindfoot is best appreciated when the foot is viewed from behind. Johnson described the so-called more-toes sign: with more advanced deformity and abduction of the forefoot, more of the lateral toes become visible when the foot is viewed from behind. The single-limb heel-rise test is an excellent determinant of the function of the posterior tibial tendon. The patient is asked to attempt to rise onto the ball of one foot while the other foot is suspended off the floor. Under normal circumstances, the posterior tibial muscle, which inverts and stabilizes the hindfoot, is activated as the patient begins to rise onto the forefoot. The gastrocnemius-soleus muscle group then elevates the calcaneus, and the heel-rise is accomplished. With dysfunction of the posterior tibial tendon, however, inversion of the heel is weak, and either the heel remains in valgus or the patient is unable to rise onto the forefoot. If the patient can do a single-limb heel-rise, the limb may be stressed further by asking the patient to perform this maneuver repetitively.
Non surgical Treatment
Get treated early. There is no recommended home treatment. While in stage one of the deformity, rest, a cast, and anti-inflammatory therapy can help you find relief. This treatment is followed by creating custom-molded foot orthoses and orthopedic footwear. These customized items are critical in maintaining the stability of the foot and ankle. Once the tendon has stretched and deformity is visible, the chances of success for non-surgical treatment are significantly lower. In a small percentage of patients, total immobilization may arrest the progression of the deformity. A long-term brace known as an ankle foot orthosis is required to keep the deformity from progressing. The Richie Brace, a type of ankle foot orthosis, shows significant success as a treatment for stage two posterior tibial dysfunction. It is a sport-style brace connected to a custom corrected foot orthodic that fits into most lace-up footwear (including athletic shoes). It is also light weight and more cosmetically appealing than traditionally prescribed ankle foot orthosis. The Arizona Brace, California Brace or Gauntlet Brace may also be recommended depending on your needs. 
Surgical Treatment
Stage two deformities are less responsive to conservative therapies that can be effective in mild deformities. Bone procedures are necessary at this stage in order to recreate the arch and stabilize the foot. These procedures include isolated fusion procedures, bone grafts, and/or the repositioning of bones through cuts called osteotomies. The realigned bones are generally held in place with screws, pins, plates, or staples while the bone heals. A tendon transfer may or may not be utilized depending on the condition of the posterior tibial tendon. Stage three deformities are better treated with surgical correction, in healthy patients. Patients that are unable to tolerate surgery or the prolonged healing period are better served with either arch supports known as orthotics or bracing such as the Richie Brace. Surgical correction at this stage usually requires fusion procedures such as a triple or double arthrodesis. This involves fusing the two or three major bones in the back of the foot together with screws or pins. The most common joints fused together are the subtalar joint, talonavicular joint, and the calcaneocuboid joint. By fusing the bones together the surgeon is able to correct structural deformity and alleviate arthritic pain. Tendon transfer procedures are usually not beneficial at this stage. Stage four deformities are treated similarly but with the addition of fusing the ankle joint.